Article Text

Abstract
Objective To determine the public's understanding of and views about a range of ethical issues in relation to death and dying.
Design Random, digit-dialling, telephone interview
Setting Ireland.
Participants 667 adult individuals.
Results The general public are unfamiliar with terms associated with end-of-life care. Although most want to be informed if they have a terminal illness, they also value family support in this regard. Most of the respondents believe that competent patients have the right to refuse life-saving treatment. Most also (mistakenly) believe that families, either alone or with physicians, have the authority to make decisions about starting or stopping treatment for incompetent patients. Most Irish people are more concerned about the quality of their dying than death itself. Religious commitment is important to most Irish people, and this impacts on their views about medical treatment and care at the end of life.
Conclusions The study paints a picture of a general public that is not very comfortable with or informed about the processes of dying and death. Great sensitivity is required of health professionals who must negotiate the timing and the context of breaking of bad news with patients and families. Educational interventions, public and organisational policies and legislation need to address the uncertainty that surrounds the role of professionals and families in making decisions for dying patients.
- Death
- attitude to death
- terminal care
- truth disclosure
- living wills
- quality/value of life/personhood
- right to refuse treatment
- elderly and terminally ill
- attitudes toward death
- living wills/advance directives
Statistics from Altmetric.com
- Death
- attitude to death
- terminal care
- truth disclosure
- living wills
- quality/value of life/personhood
- right to refuse treatment
- elderly and terminally ill
- attitudes toward death
- living wills/advance directives
Some 30 000 people die in Ireland annually,1 and 40% of these deaths occur in acute care hospitals.2 Despite this, end-of-life care is not seen as a core activity of hospitals, and it is not normally included in service plans for patients and families. Neither is its importance adequately reflected in hospital culture and organisation. In response to this, the Irish Hospice Foundation initiated the Hospice Friendly Hospitals Programme in 2007 to develop comprehensive standards for all hospitals in relation to end-of-life care and to develop the capacity of these hospitals to meet and exceed these standards. This survey is one of the measures undertaken to achieve the programme's aims, and it provides some basic information about the level of public understanding of and concerns about dying and death.
Methods
Methodology and sampling
This research involved a telephone survey of a random sample of adults. The survey was conducted by reputable market researchers (TNS/MRBI) during September 2007. Some unrelated surveys were also put to respondents during the same phone call. A sample of 1046 persons living in Ireland was contacted. Seventy-nine were <18 years and were excluded. After being informed of the subject matter, a further 300 refused to participate. This resulted in a valid sample of 667 respondents. Random digit dialling was used. Controls were imposed by region, age, sex and social class. Where discrepancies occurred, the data were weighted to ensure that the final sample was representative of the Irish adult population. The questionnaire was informed by an extensive literature review,3–16 focus group interviews17 and consultation with ethical and legal experts.
Ethical considerations
Given the sensitive nature of the topic, a number of special measures were agreed in advance to protect the rights of respondents and the integrity of the research. First, the survey was evaluated by the Clinical Research Ethics Committee of the Cork Teaching Hospitals. Full approval was granted subject to some amendments to the introduction of the survey and the provision of details of a counselling service should respondents feel distressed by the questions. Finally, the introduction to the survey specifically indicated to participants that some questions may be distressing. It was, therefore, made clear that those phoned had the right not to participate and/or to withdraw from the interview at any stage.
Results
Experience and understanding of death
Just more than one half (52%) of those who participated in the survey acknowledged that they had experienced the hospitalisation for a serious illness of a family member, relative or friend in the last 3 years, with a similar proportion (51%) having experienced the death of a family member, relative or friend during the same period. Twelve percent of the participants had been hospitalised themselves for a serious illness in the last 3 years.
Awareness of end-of-life terminology
A list of 10 terms relating to end of life was read out to respondents, and they were asked to indicate how much they knew about these terms. As table 1 illustrates, the stated awareness levels for many of the terms is quite low. Overall, the findings indicate highest awareness levels are to be found among middle-class respondents, people <65 years, females and those with the highest levels of formal education.
Awareness of end-of-life terminology
Disclosure of a terminal illness
When asked if they would like to be informed about the diagnosis of a terminal illness on their own or with someone present, most respondents (57%) said they would prefer to be told on their own, followed by 35% who would prefer to be told in the presence of their families. Four percent wanted their families told first. Just more than one (11%) in ten respondents >65 years old would prefer if the news was not disclosed to anyone, including themselves. Given the negative correlation between age and formal education,18 a similar percentage of persons with primary or no formal education also opted for non-disclosure. Those most likely to want to hear the news on their own included males, members of the farming community and those aged 45–64 years. On the other hand, 25–34-year-olds, females, housewives and people living in Leinster (Eastern region of Ireland) are most likely to want to hear the news with a family member.
Decision making in relation to terminal illness
Respondents were presented with two scenarios concerning decision making in relation to a person in a coma in the final stages of a terminal illness (figure 1). Respondents were asked to give a response for each of the four different decision-maker options: family, physician, family and physician together and courts; thus, the total of the percentages exceeds 100%.

Decision making at end of life.
The living will and its role in decision making
Just more than one fifth (22%) of the respondents acknowledged that they had told someone (eg, family or physician) how they would like to be treated if they were dying. Thereafter, a standard explanation of what constitutes a living will was relayed to respondents, and a small percentage (5%) agreed that they had drafted one. When asked to what extent they would like to be treated in accordance with a living will, respondents were divided in their opinions. The largest group (42%) would like the living will to be followed as much as possible, allowing for changes in their personal circumstances. The next largest group, comprising one quarter of all the respondents, felt it should be strictly observed, regardless of the wishes of their physician/family. Others indicated it should either be used as a reference (15%) or ignored if it was >5 years old (10%). The 34 respondents who had already made a living will responded in a similar fashion as the total group. Older respondents were most likely to want the will strictly observed.
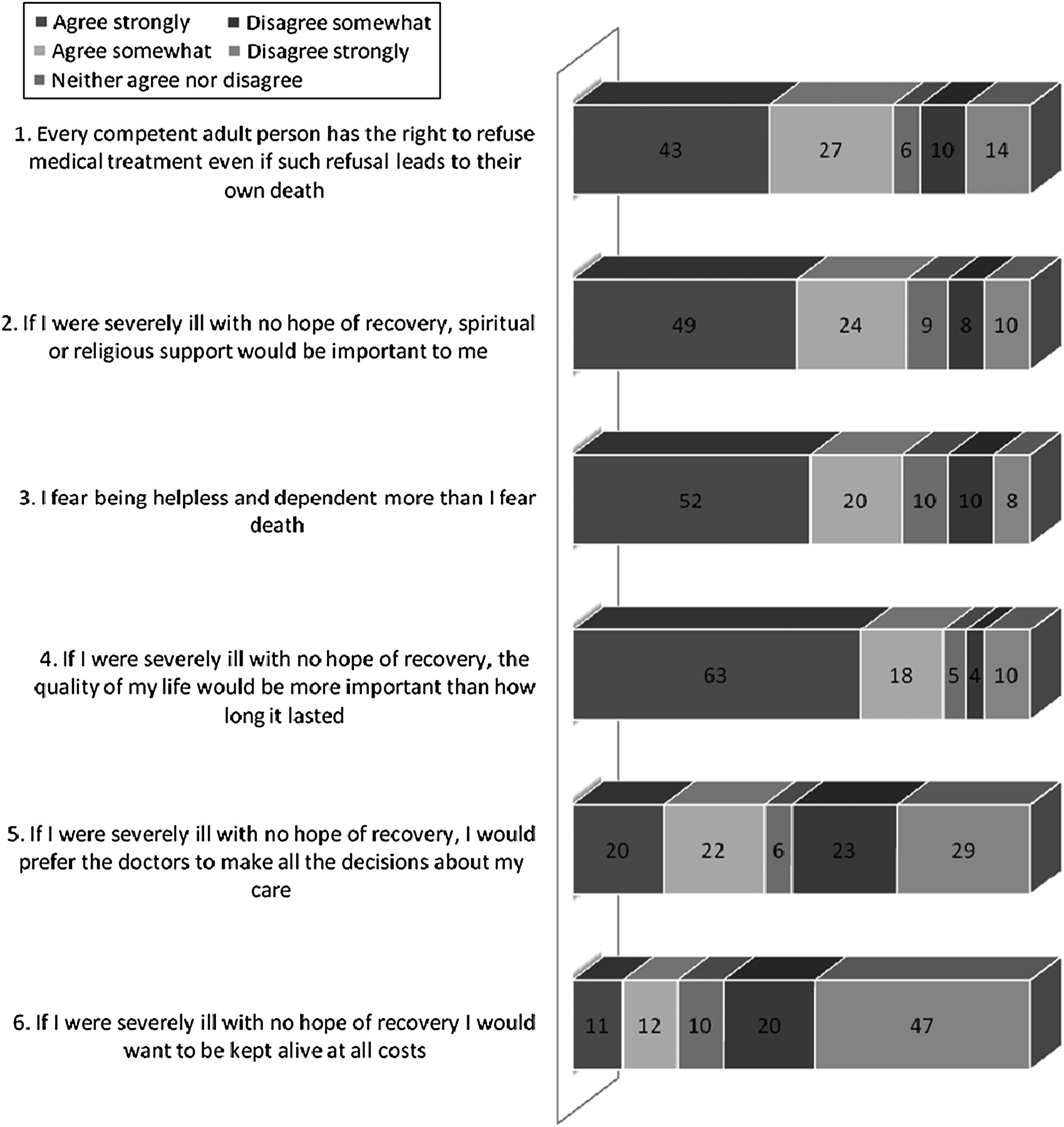
Respondents were read out a list of six statements, each reflecting an attitude relating to specific aspects of death and dying (figure 2; statements were drawn from a previous study (with authors' permission)).3 Responses to questions that probed the respondents' attitudes towards quality-of-life issues revealed that most respondents were more concerned about the quality of their dying than about death itself. In general, most people agreed that if they were severely ill with no hope of recovery, the quality of their life would be more important than how long it lasted (81%). Those who placed greatest value on length of life were most likely to be aged between 18 and 34 or >65 years.

{kind=link}
{kind=link}
Attitudes towards death and dying n=667 (answers as percentages).
Most (70%) of the respondents agreed with the statement that “every competent person has the right to refuse medical treatment even if such refusal leads to their own death”. Most agreement came from those <56 years.
That spiritual and religious support would be important attracted much agreement (73%), particularly by those >65 years. At the outset, respondents were asked, “How important are your religious beliefs to the way you live your life” and “How often, if ever, do you go to Church?” A degree of religious commitment was inferred depending on respondents' answers. In analysing responses, very religious respondents tended to agree most with statement 1, 2 and 5.
Discussion
Response rate
The response rate of 71% is roughly in line with the response rates of other Irish telephone surveys on sensitive topics. Two studies by the Royal College of Surgeons, for instance, used this methodology in their research on sexual abuse and violence in Ireland and returned similar response rates (71% and 76%, respectively).19 20 On the other hand, our study is similar in method to a UK study by Professor Irene J. Higginson in 2002.21 Higginson's report of the study does not explicitly address the response rate, but like ours, her study formed part of a national survey that included other issues. In Higginson's study, it seems that none of the 1000 adults who responded to the survey overall refused to answer the questions concerning end-of-life care. Reasons for the difference in the response rates (100% for Higginson and 71% in ours) can only be speculative; perhaps, the way in which the topic of end-of-life care was introduced to the people who participated in the survey differed. Breaking down our responses, we found that the youngest age group were most likely to refuse to participate (39%), and this is consistent with previous research in this area.22 It is also possible that a wider societal discomfort with discussing death exists: the qualitative study carried out to inform the development of the questionnaire reflected the view that death was not a matter openly discussed; one respondent summed this up stating “you know what is going to happen to you but you don't want to talk about it”.17
Experience and understanding of death
Despite the fact that more than half of the respondents had experienced the hospitalisation for serious illness and/or death of a loved one and that a tenth of them had been hospitalised themselves, the respondents largely had little or no understanding of end-of-life treatment and care terminology. This finding is consistent with other studies,7 17 one of which found the Irish public's knowledge and awareness of various bioethical areas to be quite limited in most instances, with most claiming to know “just a little or nothing” about end-of-life issues.7 Specifically, most people (71%) had never heard of the term advance directive. Although the term living will appears to be in more common parlance, nearly half of the respondents knew nothing about the term or had never heard the term before. This is consistent with earlier Irish research in this area.16 Awareness of the term postmortem was the highest among the ten terms tested. Notably, in the recent past, in Ireland, there has been much focus on the topic of postmortems since it became apparent that the organs of many deceased children had been retained after postmortem without parental knowledge. The issue culminated in a government report23 and received widespread media attention.
Information on terminal illness
International research on patients', families' and health professionals' views, experiences and practices in relation to the disclosure of bad news indicates that the Western world has seen a significant shift from a paternalistic tradition, where knowledge of and authority over medical decision making was assumed by clinicians, to a culture where patient involvement in decision making is viewed as best practice. In Ireland, several recent studies indicate that attitudes towards disclosure of bad news are changing among the general Irish population and among health professionals.8 9 16 24 The findings of this study confirm that most people, if seriously ill, would want to be told the truth about the diagnosis and the prognosis, either alone or in the presence of their families. These results are broadly similar to the results of previous Irish studies.9 25 However, it appears that some people still prefer not to be told at all of a diagnosis of serious illness. For instance, in our study, 3% of the respondents would not like the information to be told to anyone (including themselves) if they were to be diagnosed as having a terminal illness and 4% would prefer a family member to be told first. This is also consistent with national and international research9 26 27 and indicates that decisions relating to breaking bad news should be informed by patients' own preferences. One way of establishing patient preferences in this regard is to ascertain them when patients first arrive in hospital.9
Decision making on terminal illness
Most of the respondents indicated their belief that families, either alone or with physicians, have the authority to make decisions about starting or stopping treatment for incompetent patients. While Irish law supports the right of competent patients to make healthcare decisions, the public is mistaken in the belief about the rights of the families of incompetent patients. Currently, in Ireland, family members have no legal standing in relation to decision making for incompetent adults. The current legal stance is that “while hospitals may routinely seek the consent of the ‘next of kin’ in relation to healthcare decisions, this consent has no legal basis. The lawfulness of healthcare decisions about these patients depends on whether the decisions are in the best interests of the patient and, in practice, this decision devolves to the lead clinician” (Donnelly, personal correspondence, 2009). It is only when there is conflict between families and professionals that questions about end-of-life care are referred to the Irish courts.28
The lack of clear legal guidance can create difficulties for health professionals especially in situations of family conflict. However, the Law Reform Commission has recently called for the introduction of advance directives in legislation,29 30 and following on the commission's 2009 report, a mental capacity bill is due to become law in 2010, which will, hopefully, clarify who has the authority to make decisions and how those decisions might be made. In addition, recent guidelines from the Medical Council of Ireland advise physicians that advance treatment plans of patients who lack capacity should be respected if they meet certain conditions and family members may be consulted where possible.31
Meanwhile, the findings of this study underline the need to inform and educate the general public about the process of decision making in relation to incompetent patients and the need to legislate in this regard. In turn, practice and law should take into account the findings of this and similar studies that reflect people's preferences for family involvement in end-of-life decisions.
The living will and its role in decision making
Although not directly comparable, one previous Irish survey16 found that 14% of Irish adults have told someone where they would like to be treated if they became terminally ill (eg, hospital, home, hospice), 21% had told someone what they would like at their funeral and 46% had told someone whether they would like to be buried or cremated. Previous surveys on the topic of living wills or advance directives suggest that the 5% of our respondents who acknowledged that they had written a living will is relatively low. In 2004, for instance, 14% of a representative sample of the Irish public stated they had written an advance directive or living will,16 and 11% of the participants in a 2007 Irish Council for Bioethics consultation said they had actually written up a document concerning their future medical care.8 A question in the Irish Council for Bioethics (2005) survey found that 39% of Irish adults strongly agreed with the statement “Advance directives should be legally binding in all circumstances and take precedence over the wishes of a patient's next of kin and their physician's advice”.7 Others were less sure of what the legal standing of an advance directive should be. However, caution should be exercised in making direct comparisons owing to differences in wording and methodology across the three surveys. Given that nearly half of the respondents to our survey knew little or nothing about living wills and most of them had never heard of the term advance directive, it is not surprising that so few had actually completed one.
As indicated in the previous section on decision making, living wills do not, currently, have any status in Irish law, and their uncertain status may explain why so few people in Ireland think that they might be important to complete. It is to be hoped that increased awareness and the eventual introduction of legislation giving legal status to advance directives will encourage the general public to consider the role of planning in the care of dying patients.
Attitudes towards death and dying
Most of the respondents agreed that competent individuals have the right to refuse medical treatments even if this decision results in their death. Most of the respondents also placed emphasis on the quality of their life rather than on its length, and they indicated that they feared being helpless and dependent more than they feared death. Both these responses mirror results previously obtained in the UK in response to identical questions.4 However, when correlated with age, the findings indicate that more of the very old and the very young want to be kept alive at all costs. The reasons for the age differential are unknown. Given that younger people were more likely to refuse to participate at all in the survey, it is possible that they have not seriously considered the process of dying and death and, so, cannot imagine circumstances where life would not be preferable to death. It is possible that religious belief may be an influencing factor for the older group. That spiritual and religious support would be important attracted a large amount of agreement particularly by those aged >65 years and is again in line with the results obtained in the UK.4 Although one previous study found that there was a relationship between certain death-related attitudes and church attendance in the UK,32 the impact of religion on end-of-life beliefs has never been explored in an Irish context. In our study, the correlation between respondents' level of religious commitment and their responses to the attitudinal statements indicate that those who are religiously committed place a high value on life, reject the right to refuse treatments that might forestall death, respect medical authority and value spiritual support in their end-of-life care. The age stratum is representative, and no significant differences emerged for the middle-aged group. Considering that 3.9 of 4.2 million people supplied a religion in the 2006 Irish population census and that 87% of respondents in our study stated that religious beliefs were important to them, the impact of religious belief on death-related attitudes in Ireland presents an important area for further research.
Conclusions
This is one of the few national studies pertaining to end-of-life care that has been undertaken in Ireland. It is also the first national telephone survey with a focus on ethical issues that arise at the end of life. Given that the sample surveyed was representative of the general population and that the study's findings are consistent with related research undertaken in Ireland, confidence can be placed in the representativeness of the survey results.
On the other hand, although elements of the questionnaire were tested before (eg, the attitudinal questions),3 the questionnaire, as a whole, was not tested for validity and reliability beyond an appeal to experts in the field.
The first conclusion that can be drawn from the survey's results is that the lack of familiarity with terms used in relation to end-of-life treatment and care places an onus on state agencies and professional bodies to ensure that basic information about end-of-life care is communicated in a meaningful way to the general public.
Second, it is clear that Irish people, like most people in similar studies worldwide, want to be told the truth if they have a terminal illness. Although many welcome family support, they rarely want their families informed of the illness first. This study also confirms the existence of a minority who do not want to be told bad news. It follows that great sensitivity is required of health professionals in negotiating the timing and the context of breaking of bad news.
Third, this study shows that many Irish people, particularly older people, place a great deal of trust in their physician when decisions must be made about their care. Most agreed that competent persons had the right to refuse medical treatment, but a sizable number also seemed unclear as to who has the authority to make decisions for incompetent patients. Again, there seems an onus on professionals and hospitals to ensure that patients and their families are aware of the processes of decision making for competent and incompetent patients and the role that each individual might have in any deliberations. In turn, given the lack of clear legal guidance in relation to decision making for incompetent patients, it seems imperative that the government act to address this uncertainty. The same could be said in relation to advance directives.
Finally, the findings suggest that most people are more concerned about the quality of their dying than death itself. Reasons for holding particular attitudes towards the dying process are unknown. This survey indicates, however, that religious commitment is important to most Irish people and that this impacts on their views about medical treatment. On the other hand, it is important to note that a sizable minority did not place importance on spirituality at the end of their lives.
In sum, our study paints a picture of a general public that is not very comfortable with or informed about the processes of dying and death. Uncertainty about who decides what and when coexists with trust in medical professionals and family members when important decisions need to be made. For some, faith in God and in other authorities might go some way towards filling the void that has been created by the lack of discussion, policy and law pertaining to the process of dying and death. However, the results of the study, overall, underline the need for educators, health professionals and other stakeholders to raise awareness and deepen understanding of this neglected but inevitable stage of human life.
References
Footnotes
Funding This study was funded by the Irish Hospice Foundation.
Competing interests None.
Ethics approval This study was conducted with the approval of the clinical research ethics committee of the Cork Teaching Hospitals.
Provenance and peer review Not commissioned; externally peer reviewed.
Other content recommended for you
- Importance of the advance directive and the beginning of the dying process from the point of view of German doctors and judges dealing with guardianship matters: results of an empirical survey
- A survey of the perspectives of patients who are seriously ill regarding end-of-life decisions in some medical institutions of Korea, China and Japan
- Examining the ethico-legal aspects of the right to refuse treatment in Turkey
- When enough is enough; terminating life-sustaining treatment at the patient's request: a survey of attitudes among Swedish physicians and the general public
- Emergency clinicians' attitudes and decisions in patient scenarios involving advance directives
- Survey on advance care planning of Italian outpatients on chronic haemodialysis
- The do-not-resuscitate order: associations with advance directives, physician specialty and documentation of discussion 15 years after the Patient Self-Determination Act
- When slippery slope arguments miss the mark: a lesson from one against physician-assisted death
- Practising what we preach: clinical ethicists’ professional perspectives and personal use of advance directives
- Clinical ethical dilemmas: convergent and divergent views of two scholarly communities